
Life in Motion Chiropractic · Livonia, MI
“Hip pain” is often not
coming from the hip.
The sacroiliac joint — where your spine meets your pelvis — is one of the most commonly misdiagnosed pain sources in the body. It mimics hip pain, low back pain, and sciatica. Dr. Dockery’s exam identifies exactly which structure is involved before any treatment begins.
What is the sacroiliac joint — and why does it cause so much confusion?
The sacroiliac joint sits at the base of the spine, where the sacrum — the triangular bone at the bottom of the vertebral column — connects to the iliac bones of the pelvis. You have two of them, one on each side, and together they transfer load between the upper body and lower limbs with every step you take.
The SI joint is designed to move very little — typically just 2–4 millimeters of gliding motion. But that small amount of movement is essential. When the joint becomes restricted (hypomobile), inflamed, or excessively mobile (hypermobile), it generates a distinctive pain pattern that is frequently mistaken for something else entirely — most commonly lumbar disc disease, hip bursitis, or sciatica.
Why the confusion? The SI joint refers pain to the same areas as several other structures: the lower back, the buttock, the outer hip, and even the back of the thigh. Without specific clinical provocation testing, it’s easy to chase the wrong diagnosis — and treat the wrong thing — for months or years.
The clinical test that changes everything: SI joint dysfunction is diagnosed through a cluster of specific provocation tests — FABER, Gaenslen’s, thigh thrust, distraction, and compression. When three or more of these tests are positive, the research supports SI joint dysfunction as the primary pain generator with high clinical confidence. This is part of every pelvic and hip evaluation at Life in Motion. Learn what your first visit includes →
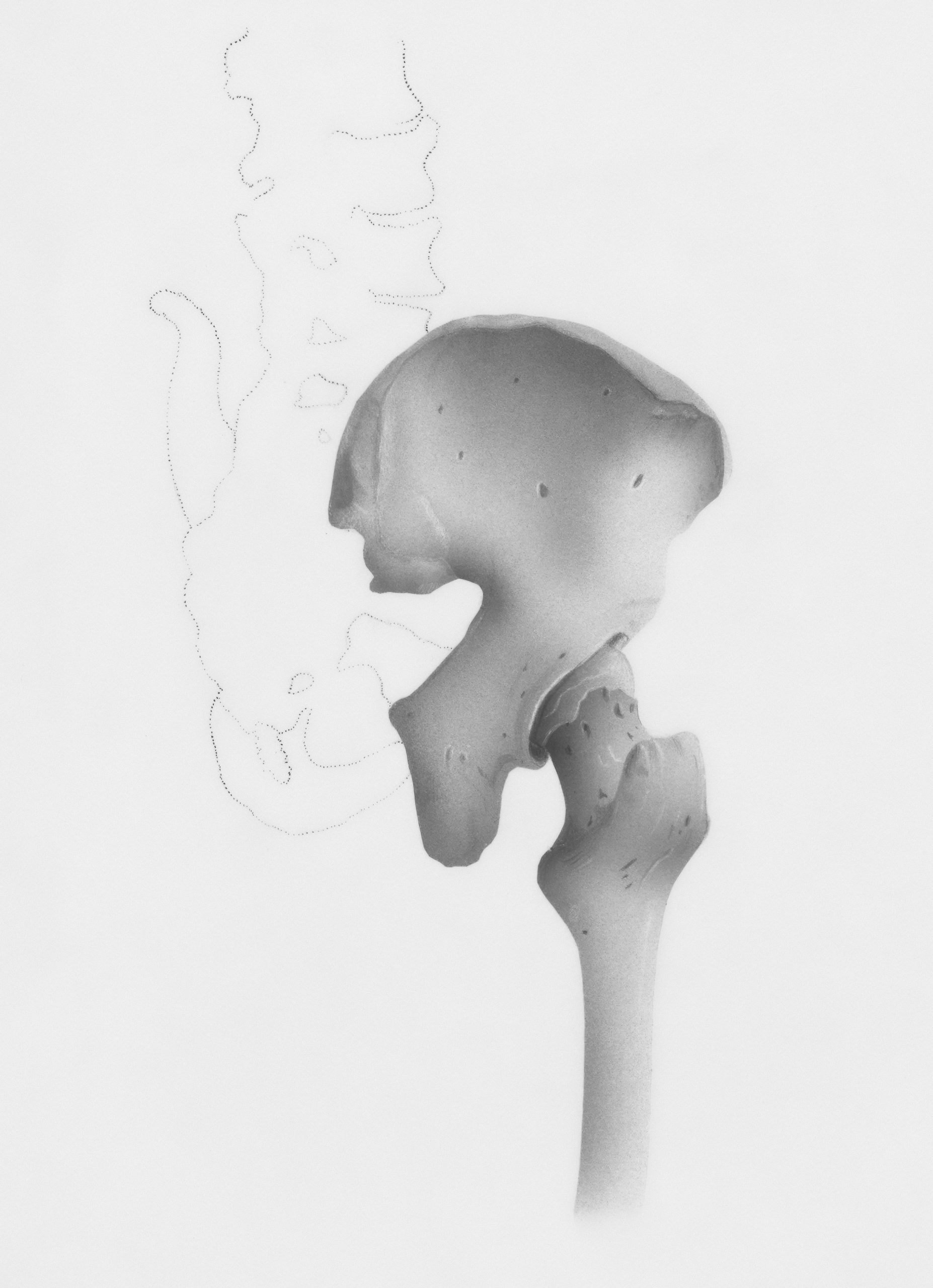
The sacroiliac joint connects the sacrum (base of the spine) to the iliac bones of the pelvis on both sides — a weight-bearing joint that transfers load with every step.
SI joint pain vs. hip joint pain — how to tell the difference
Because both structures refer pain to the same general region, patients and even clinicians frequently confuse them. Here’s how the presentations typically differ — and why the distinction matters for treatment.
- Deep aching pain in the lower back, buttock, or outer hip — usually on one side
- Worsens with prolonged standing, walking, or transitioning from sitting to standing
- Pain with rolling over in bed or putting weight on one leg (climbing stairs, dressing)
- May refer down the back of the thigh — rarely past the knee
- Often associated with a sensation of pelvic instability or “giving way”
- Improved (temporarily) by changing positions frequently
- Sometimes worsens with lumbar extension or twisting away from the painful side
SI joint pain is often diagnosed late because it mimics disc and facet pain so closely. Specific provocation testing is essential to identify it.
- Deep groin pain or anterior (front of) hip pain — the classic “true hip joint” location
- Pain with hip rotation, especially internal rotation and end-range flexion
- Worsens with impact activities — walking long distances, running, stairs
- May produce a catching, clicking, or locking sensation in the hip joint
- Can refer to the front of the thigh or the knee
- Often associated with hip stiffness on waking and improvement with movement (osteoarthritis pattern)
- Restricted passive range of motion — particularly flexion, abduction, and internal rotation
True hip joint pathology (osteoarthritis, labral tears, FAI) typically requires imaging for definitive diagnosis. Clinical exam guides appropriate referral when needed.
The honest reality: Many patients have both. The SI joint and hip joint are anatomically adjacent and mechanically interdependent — dysfunction in one frequently contributes to dysfunction in the other. Dr. Dockery’s pelvic evaluation assesses both simultaneously so nothing is missed.
Hip and pelvic conditions treated at Life in Motion
From SI joint dysfunction to hip impingement, piriformis syndrome to bursitis — each of these responds to a different treatment approach, which is why accurate diagnosis comes first.
SI Joint Dysfunction
Hypomobility, hypermobility, or inflammation of the sacroiliac joint causing lower back, buttock, and referred leg pain. The most commonly undertreated source of chronic pelvic and hip-region pain — and one of the most responsive to chiropractic care.
Hip Osteoarthritis
Age-related degeneration of the hip joint cartilage producing groin pain, stiffness, and progressive loss of mobility. Conservative chiropractic care and laser therapy manage symptoms, preserve function, and support joint health — often delaying or reducing the need for surgical intervention.
Piriformis Syndrome
Irritation or spasm of the piriformis muscle — deep in the buttock — compressing the sciatic nerve and mimicking both sciatica and SI joint pain. Frequently misdiagnosed because it presents like a disc problem but has a distinct muscular source.
Hip Bursitis (Trochanteric)
Inflammation of the bursa at the outer hip, producing sharp or burning pain along the lateral hip and thigh — often worse when lying on the affected side. Responds well to soft tissue treatment, laser therapy, and activity modification.
Femoroacetabular Impingement (FAI)
Abnormal contact between the femoral head and acetabulum during hip movement — producing groin pain and restricted internal rotation, especially in active patients. Conservative care addresses muscular imbalance and movement patterns; referral is coordinated when surgical evaluation is indicated.
Pelvic Girdle Pain & Instability
Pain and instability across the pelvis — including the pubic symphysis and both SI joints — common during and after pregnancy as a result of hormonal ligament laxity. Responds well to targeted pelvic stabilization, gentle manipulation, and core rehabilitation.
“The SI joint is involved in more cases of low back and hip pain than most patients — or providers — realize. When the right test is applied to the right joint, the diagnosis often becomes clear within minutes. The challenge is knowing to look for it.”
Our approach to hip & SI joint relief
Every treatment plan at Life in Motion begins with an accurate diagnosis. Once the involved structures are clearly identified, care is targeted specifically at them — not at the general region of pain.

SI Joint Manipulation & Pelvic Adjustment
Specific sacroiliac joint manipulation restores proper joint mobility, reduces nerve irritation, and addresses the muscular guarding patterns that form around a dysfunctional SI joint. Dr. Dockery is trained in multiple SI joint techniques — from traditional diversified adjusting to low-force instrument-assisted approaches — ensuring the method always matches your presentation, comfort level, and acuity of symptoms.
Learn about our chiropractic techniques →
Class 4 Laser Therapy
Our LightForce Class IV laser penetrates deep into the pelvic joints and surrounding soft tissue to reduce inflammation in the SI joint capsule and surrounding ligaments, release tight piriformis and gluteal musculature, and accelerate tissue repair. Particularly effective for patients with active SI joint inflammation, hip bursitis, and piriformis syndrome — where reducing the inflammatory load is a critical first step before rehabilitation can begin.
Learn about Class 4 Laser Therapy →
Soft Tissue Release & Myofascial Work
The piriformis, gluteus medius, iliotibial band, and hip flexors are the primary soft tissue drivers of hip and SI joint pain. Targeted myofascial release and trigger point therapy to these muscles reduces the tensional load on the SI joint, releases nerve entrapments (particularly the sciatic nerve in piriformis syndrome), and restores the movement quality that keeps symptoms from recurring.
Learn about massage therapy →Pelvic Stabilization & Glute Rehabilitation
SI joint dysfunction is almost always accompanied by weakness or poor motor control in the gluteus medius, deep core stabilizers, and hip external rotators — the muscles responsible for controlling pelvic alignment under load. Without addressing this, symptoms return no matter how well the joint is adjusted. Dr. Dockery prescribes evidence-based pelvic stabilization and glute activation exercises specific to your exam findings, available to review at home through our Rehab Exercise Library.
Hip and SI joint pain affects a wide range of patients
The common thread is pain in the lower back, hip, or buttock that hasn’t fully responded to treatment — because the source hasn’t been accurately identified yet.
Patients diagnosed with “lower back pain” or “sciatica” who have not responded to standard lumbar treatment
Runners, cyclists, and athletes with persistent hip, buttock, or IT band pain that limits training
Pregnant or postpartum patients experiencing pelvic girdle pain, SI joint instability, or pubic symphysis dysfunction
Patients who sit for long periods — drivers, office workers — who develop one-sided hip and buttock pain
Post-lumbar fusion patients whose pain has shifted to the SI joint due to altered load transfer
Auto accident patients with pelvic, hip, or sacral pain following a collision
Is chiropractic effective for SI joint dysfunction?
Yes — and chiropractic care is consistently recognized as a first-line conservative treatment for sacroiliac joint dysfunction in clinical guidelines. The research supports both the accuracy of clinical provocation testing for diagnosis and the effectiveness of spinal manipulation for treatment.
A systematic review published in the European Spine Journal found that manipulation of the sacroiliac joint significantly reduces pain intensity and improves functional outcomes compared to no treatment or passive modalities alone — with effects maintained at short- and medium-term follow-up.
The International Association for the Study of Pain (IASP) and the North American Spine Society (NASS) both recommend conservative care — including manipulation and exercise — as the preferred approach for SI joint pain prior to interventional or surgical options.
Key Clinical Finding — Diagnosis
A landmark study by Laslett et al. (2005) established that a cluster of five SI joint provocation tests (distraction, thigh thrust, Gaenslen’s, compression, and sacral thrust) produces high sensitivity and specificity for SI joint dysfunction when three or more are positive. This diagnostic protocol is used at Life in Motion as part of every pelvic evaluation.
This matters clinically: without these tests, SI joint dysfunction is routinely misattributed to lumbar disc or facet pathology — leading to months of misdirected treatment.
Laslett M, et al. “Diagnosis of sacroiliac joint pain: validity of individual provocation tests and composites of tests.” Manual Therapy. 2005;10(3):207–218. PubMed ReferenceWhat patients say about care at Life in Motion
I came in with intense SI joint pain, and from the first visit Dr. Dockery was incredibly thorough — he explained what was going on, adjusted me with care, and gave me the right exercises. I noticed real improvement quickly. He treats the root of the issue and empowers you with the tools to heal. The entire staff is welcoming and professional.
My treatment plan is tailored to my specific needs with clear, measurable goals so I can actually see my progress. I’d never been to a chiropractor before — Dr. Dockery exceeded all my expectations.
Dr. Dockery is knowledgeable, professional, and kind. More than once, he’s restored my freedom of movement and quality of life. I would recommend him to my own family and friends.
Dr. Dockery is outstanding. You can tell he truly cares. He takes the time to teach and never stops learning. I always leave with useful information and exercises to support my recovery.
Read more patient testimonials →Hip & SI joint pain FAQs
How do I know if my hip pain is coming from the SI joint?
SI joint pain typically presents as a deep ache in the lower back, buttock, or outer hip — usually on one side. It tends to worsen with transitioning from sitting to standing, prolonged walking, climbing stairs, or rolling over in bed. Pain that wraps around the front of the hip or groin suggests the actual hip joint instead. A clinical exam using SI joint provocation tests is the definitive way to differentiate the two — and that’s exactly what your first visit includes. Learn what to expect →
Can a chiropractor fix SI joint dysfunction?
Yes. Chiropractic care is widely considered a first-line conservative treatment for SI joint dysfunction. Specific sacroiliac joint manipulation restores proper joint mobility, reduces inflammation, and relieves the muscle guarding that perpetuates SI pain. Combined with targeted rehabilitation for the glutes, core, and hip stabilizers, most SI joint cases resolve or significantly improve with conservative care.
Is SI joint pain the same as sciatica?
No — but they’re frequently confused. True sciatica originates from sciatic nerve compression in the lumbar spine, typically producing pain, numbness, or tingling that travels below the knee into the foot. SI joint pain can refer down the back of the thigh but rarely travels below the knee, and it does not produce neurological symptoms like foot numbness or reflex changes. Piriformis syndrome — a close cousin of SI joint dysfunction — can also compress the sciatic nerve and mimic both. A thorough exam differentiates all three clearly. Learn more about sciatica →
What causes the SI joint to become painful?
Common causes include leg length discrepancy, prolonged asymmetric sitting or driving, pregnancy-related pelvic ligament laxity, weak glute and core muscles that force the SI joint to absorb excess load, prior lumbar spine fusion (which transfers stress to the SI joint), and direct trauma from falls, auto accidents, or sports injuries. Identifying which factor is primary in your case shapes the treatment approach significantly.
I had a lumbar fusion. Could my new pain be the SI joint?
Very possibly. Adjacent segment disease — where spinal fusion transfers mechanical load to the next structure down — is a well-documented phenomenon, and the SI joint is the most common recipient of that transferred stress after lumbar fusion. Studies suggest that up to 75% of patients who develop new pain after lumbar fusion may have concurrent SI joint dysfunction. This is a presentation Dr. Dockery assesses specifically.
Do you accept insurance for hip and SI joint treatment?
Yes, we accept most major insurance plans. Check your coverage here →
Clinical References & External Resources
- Laslett M, et al. “Diagnosis of sacroiliac joint pain: validity of individual provocation tests and composites of tests.” Manual Therapy. 2005;10(3):207–218. PubMed
- Simopoulos TT, et al. “A systematic evaluation of prevalence and diagnostic accuracy of sacroiliac joint interventions.” Pain Physician. 2012;15:E305–E344. Pain Physician
- Buchbinder R, et al. “Hip osteoarthritis.” BMJ. 2008;336:1107. BMJ
- North American Spine Society. “Evidence-Based Clinical Guidelines for Multidisciplinary Spine Care: Diagnosis and Treatment of Low Back Pain.” NASS Clinical Guidelines
- American Academy of Orthopaedic Surgeons. “Hip Pain and Problems.” AAOS OrthoInfo
If your hip or back pain hasn’t responded, the source may not have been found yet.
Same-day and Saturday appointments available. Dr. Dockery’s comprehensive pelvic and hip evaluation starts at your first visit.
27620 Five Mile Rd, Livonia, MI 48154 · Mon–Thu & Saturday by Appointment