
Modified Side Bridge
with Hip Transition
A lateral hip and core stability exercise prescribed by Dr. Dockery that combines a modified side plank hold with a controlled hip abduction transition — training the glute medius, lateral core, and quadratus lumborum together in a position that directly transfers to standing, walking, and single-leg stability.
What Is the Modified Side Bridge with Hip Transition?
The Modified Side Bridge with Hip Transition is a two-phase lateral stability exercise that begins with a side-lying plank supported on one forearm and bent knees (the “modified” position), then adds a controlled hip abduction lift of the top leg as a transition — challenging both the lateral core and the glute medius in a single integrated movement.
The exercise earns its name from the combination of the modified side bridge (a side plank variation that reduces demand compared to the full straight-leg version, making it accessible for patients early in rehabilitation) and the hip transition (the controlled lifting and lowering of the top hip/leg that challenges the glute medius at the end range of its function).
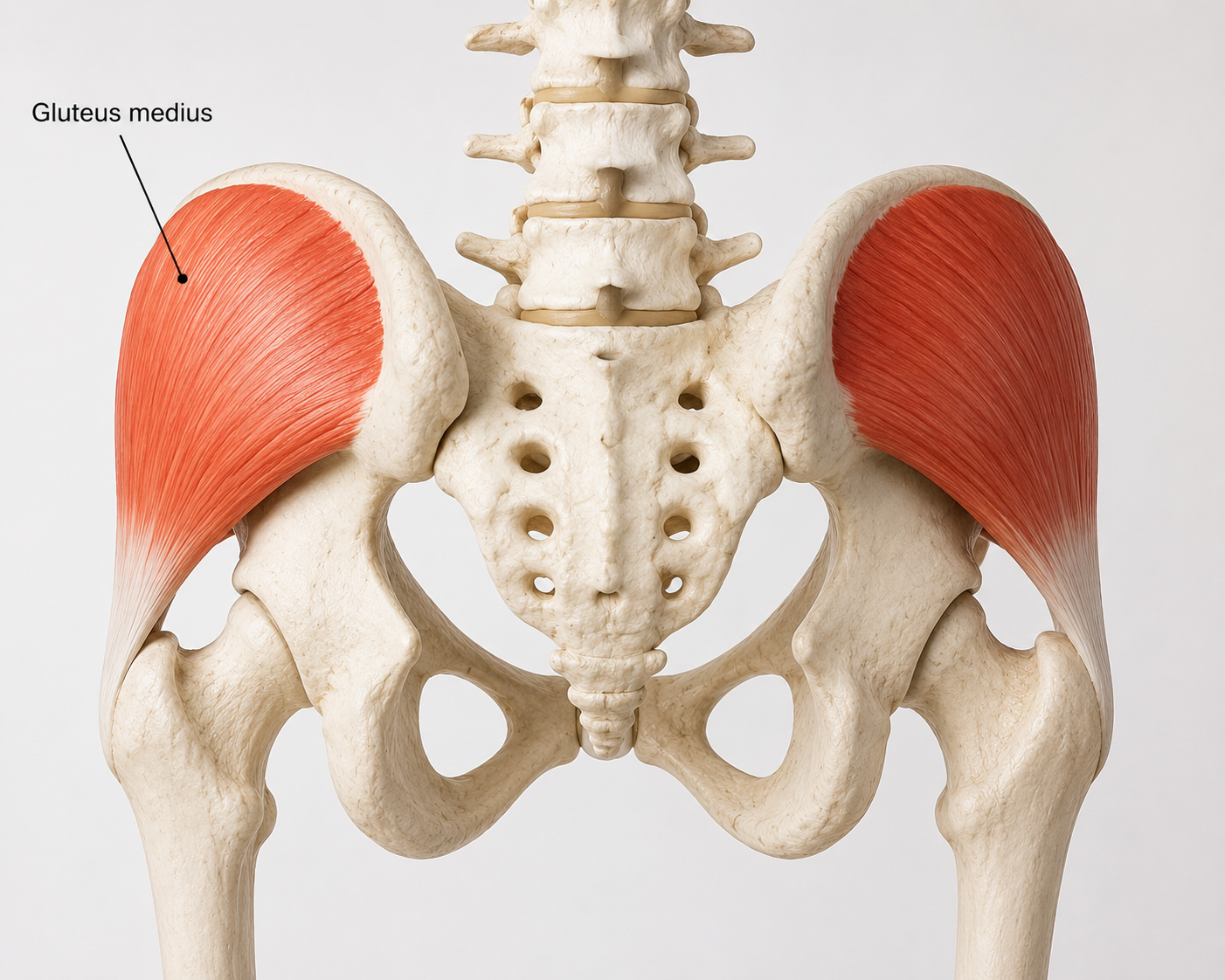
The gluteus medius is the primary target — a fan-shaped muscle on the outer surface of the pelvis that stabilizes the hip during single-leg loading, controls pelvic drop during walking and running, and prevents the inward knee collapse that drives patellofemoral pain, IT band syndrome, and hip dysfunction. According to Physiopedia’s review of gluteus medius function, weakness of this muscle is among the most consistently identified contributors to lower extremity injury and low back pain — yet it is frequently undertrained because standard hip exercises preferentially recruit the gluteus maximus and TFL instead.
The modified side bridge position specifically isolates the glute medius by placing the hip in a position where the gluteus maximus and TFL are mechanically disadvantaged, making it one of the most targeted glute medius exercises available without equipment.
Primary muscles trained: Gluteus medius (hip abduction and pelvic stability), quadratus lumborum (lateral trunk stabilization), and obliques (anti-lateral-flexion core control). Secondary: gluteus minimus, TFL, hip abductor complex. The exercise trains all of these simultaneously in a gravity-loaded side-lying position that mimics single-leg stance demands.
Clinical note: This exercise sits in the middle of the lateral hip progression: it follows the Banded Clam (glute medius in a lower-demand non-weight-bearing position) and precedes single-leg balance and lateral band walking. For patients with Trendelenburg gait, IT band syndrome, or SI joint pain with lateral hip weakness, the modified side bridge with transition is often the single most important exercise in the program.
Common Conditions This Exercise Addresses
Understanding the Exercise Structure
Modified side plank
Supported on one forearm and the bottom knee, with the top leg extended or stacked on the bottom knee. Hips lifted off the floor, body forming a straight line from head to knee. This isometric hold loads the lateral core and glute medius before any movement is added.
Controlled top-leg abduction
While maintaining the bridge position and spinal alignment, the top leg is lifted (abducted) in a controlled arc and then lowered back to the starting position. This dynamic phase challenges the glute medius through its full abduction range while the lateral core maintains anti-lateral-flexion stability.

Step-by-Step Instructions
Set up the side-lying starting position
Lie on your side with your bottom forearm on the floor, elbow directly under your shoulder. Bend both knees to approximately 45–90 degrees, stacking the feet. Your body should be in a straight line from head to knees when viewed from behind. Place the top hand on your hip or in front of you for balance.
Lift into the modified side bridge
Press through the forearm and the bottom knee to lift the hips off the floor. The goal is a straight, neutral line from the head through the hip — avoid sagging the hips toward the floor or hiking them toward the ceiling. Feel the lateral core engage to maintain the position. Create light abdominal pressure before lifting to stabilize the spine.
Hold and establish the bridge position
Before adding the hip transition, hold the bridge position for 2–3 seconds to ensure spinal alignment and core engagement are established. The shoulder should be stacked over the elbow, the neck neutral, and the hips level. Do not proceed to the transition if you cannot maintain this alignment.
Perform the hip transition
While maintaining the bridge position and keeping the pelvis completely still, lift the top leg upward in a controlled abduction arc — approximately 30–45 degrees from the bottom leg. Keep the toes pointing forward (not toward the ceiling, which rotates the hip and recruits the TFL instead of the glute medius). Pause briefly at the top.
Lower the leg with control and repeat
Lower the top leg back to the starting stacked position slowly and under control — the eccentric lowering phase is as important as the lift for building glute medius strength and stability. Complete the prescribed repetitions on one side before switching to the other.
Lower the hips and rest between sets
After completing the set, lower the hips back to the floor with control. Do not collapse — lower slowly to maintain core engagement through the full set. Rest briefly before the next set or switching sides.
Most common compensation: Allowing the hips to sag or rotate during the leg lift. If the pelvis rotates backward when you lift the top leg, the hip flexors (not the glute medius) are doing the work. Keep the toes pointing forward throughout the lift, and if the pelvis moves during the transition, reduce the range of the leg lift until glute medius strength improves. The hip staying completely still is more important than lifting the leg high.
Key Technique Points
Watch the Technique
Why This Exercise Works
Frequently Asked Questions
This content is for educational purposes only. Stop if symptoms worsen or pain develops, and consult Dr. Dockery if you are unsure whether this exercise is appropriate for your condition.
Build Lateral Hip Strength in Livonia, MI
The Modified Side Bridge with Hip Transition is most effective as part of a complete glute medius and lateral stability program. Dr. Dockery serves patients throughout Livonia, Farmington Hills, Redford, Plymouth, and greater Wayne County.